If you thought MAID was as bad as it could get, you would be wrong. We are also transplanting the organs of people killed in hospitals. Next step: allowing those euthanized at home to be transferred to the hospital to harvest their organs.
This is from the Canadian Medical Association: Deceased organ and tissue donation after medical assistance in dying: 2023 updated guidance for policy
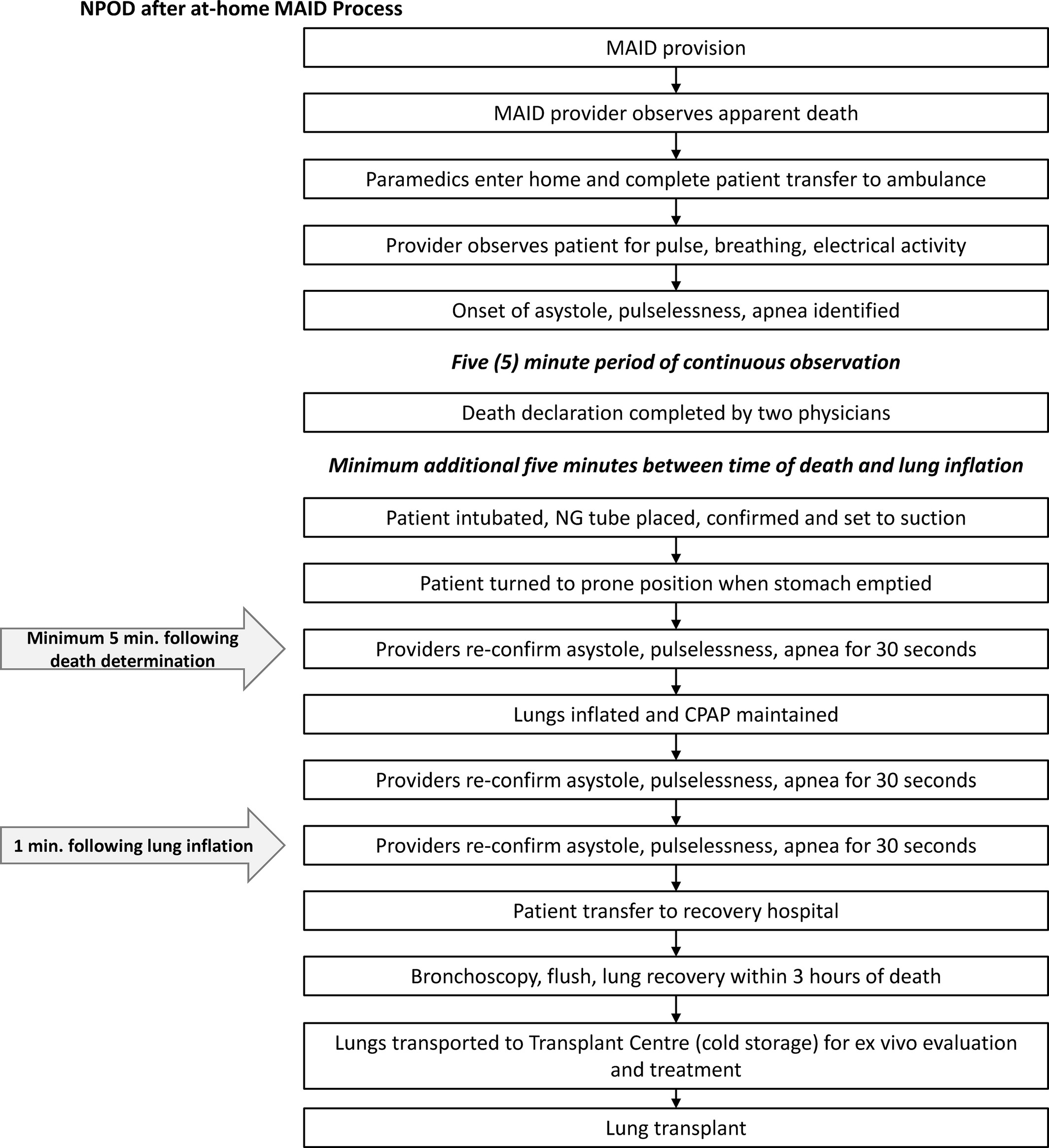
"In a case in Ontario, the patient received the MAiD procedure at home.16 When the family was ready, the patient was transferred to an ambulance, where death was confirmed. Intubation was performed and an orogastric tube was secured [This is to empty the contents of the stomach of the dead person] before the patient was placed prone on the ambulance stretcher. The rest of the protocol for lung protection during the absence of circulation was applied before the patient was transferred to the hospital for organ recovery.17“
(16. Organ donation after medical assistance in dying (MAID) has only been possible for patients having the MAID procedure performed at a hospital facility due to prohibitive warm ischemic times. Herein, we describe a protocol for lung donation following MAID at home and demonstrate excellent postoperative outcomes. Lung donation following MAID at home is possible and should be considered by transplant programs.)
Note these troubling remarks in the guidelines:
"This guidance does not address the ethics of MAiD, questions regarding eligibility or assessment for MAiD, or provision of MAiD. It focuses on organ donation for those patients who have been assessed and found eligible for MAiD through established processes in Canada." (emphasis added)
And this:
"international experience with donation after MAiD is limited, and therefore, we found limited data to inform our recommendations. There was potential bias among forum participants, given that they were generally supporters of the current deceased donation and transplantation system, as well as donation after MAiD. (emphasis added)
Of course there was bias in this exercise, since everyone involved were MAID supporters, including MAID patients and family partners who were included as participants for the forum.
Yet strangely, the authors actually do mention the ethical challenges of organ donation after MAID:
"The purpose of this updated guidance is to continue to inform the development of policies and practices of donation after MAiD. This will help clinicians navigate the medical, legal and ethical challenges that arise when they support patients pursuing donation after MAiD."
So how do we manage to kill someone at home, and successfully extract their lungs for transplant? Well, we have a flow chart for that:
1) First we kill the patient. Make sure patient is dead.
2) Paramedics transfer (dead) patient to the ambulance.
3) Next we pump the (dead) patient's stomach to remove messy contents. Reconfirm (dead) patient is dead.
4) Inflate lungs.
5) Reconfirm (dead) patient is dead. (Do this multiple times. Just to make sure dead patient is truly dead. Just to be sure.)
6) Transfer (dead) patient to hospital.
7) Recover lungs at hospital.
"CASE REPORT
In advance of his death, the donor provided written consent to describe the details of his case.
A 48-year-old man with Huntington's disease was referred to TGLN by the patient's MAID provider. He understood that at this time only lungs and tissues could be donated if he died at home but he did not wish to die in the hospital. Consent to organ donation after MAID at home was provided. Following confirmation of medical suitability, a date and time for MAID were obtained.
Unfractionated heparin (1000 units per kg) was administered 5 minutes prior to the procedure. The MAID combination of medications resulted in sedation (midazolam), local anesthetic effect on the vein (lidocaine), the induction of general anesthesia (propofol), muscle paralysis (rocuronium), and cardioplegia (concentrated potassium chloride) leading to virtually immediate cardiac arrest. The family was prepared to spend some time with the body after death. When the provider and family were ready, the patient was transferred to a pre-arranged ambulance and attached to a cardiac monitor. Apnea, pulselessness, and asystole were observed for 5 minutes. Death was declared by the MAID provider and confirmed by a second physician, as required by law.
The patient was then intubated, an orogastric tube was secured, and the patient was placed prone on the ambulance stretcher. After a minimum of 10 minutes, the lungs were inflated to a continuous positive airway pressure of 20 cm H2O using medical air and asystole once again was confirmed. The protocol of lung protection during the absence of circulation was developed within our uncontrolled DCD program and proven to be feasible.5 Nonurgent transport to the hospital ensued. Given that this patient was a police officer, an unplanned police escort and honor guard was provided en route to the hospital and operating room.
The lung retrieval team recovered the organs in standard fashion. Time from cardiac arrest to flush of the organ was 62 minutes. Lungs were transferred to Toronto General Hospital and ex vivo lung perfusion for 3 hours and 47 minutes confirmed excellent lung function (Table 1). Total preservation time from cold flush in the donor to reperfusion in the recipient was 12:27 and 15:29 hours for the first and second lungs, respectively.
The recipient was a 68-year-old woman with end-stage lung disease from interstitial lung disease. She was small for the donor lungs and thus bilateral lower lobe transplantation was performed on central venoarterial extracorporeal membrane oxygenation (ECMO). Due to preexisting donor-specific antibodies, intraoperative plasmapheresis was performed prior to lung reperfusion as part of our clinical protocol.7 Separation from ECMO was uneventful and the patient was extubated 8 hours following transplant. She was briefly reintubated overnight on postoperative day (POD) 12 for clearance of a mucus plug by bronchoscopy and was discharged home on POD."
No comments:
Post a Comment